Ergonomic analysis of the tasks of endosurgery helps in the design of instruments and tasks, and in decreasing the mismatch between human capacities and technology. It requires the study of the constraints of working through narrow fixed ports and an understanding of how the processes of gripping and dividing tissue are determined by its mechanical properties.
This formal approach may offer more than trial-and-error evolution and haphazard solutions to problems by quicker general answers, with shorter learning curves, greater productivity and fewer errors, and decreased operator frustration. The first and ultimate benefit is for patients undergoing endosurgery.
Keywords: endosurgery, engineering, ergonomics, laparoscopic, surgery, systems.
Compared with open surgery, endosurgery presents special constraints and difficulties. A new surge of surgery was driven by the emergence of new technology and the commercial availability of the 'camera on a chip'. Instrument manufacturers tried hard to meet the new constraints that emerged at the same time. This was reflected in the rapid appearance of new generations of instruments. Surgeons and engineers responded by attempting to analyse generic features of this new discipline 1 , and by continually modifying new techniques, but with incomplete success.
There is a close parallel with the emergence of microsurgery in the 1970s.
For the early part of that decade the half-life of new developments was
about the same as the interval between major international conferences
in the field, about six months. The preoccupations of microsurgery were
seeing fine detail, dissecting and suturing fine tissue, and control of
fine movement. Some of the answers were provided by engineering. A few
of the solutions were based on principles of ergonomics, whether by intuition
and trial-and-error or formally under that name 2,3 (Table
1).
Table 1. History of applying ergonomics to microsurgery
| Basis |
Working with smaller structures
|
||
Problem |
Surgical responses | Engineering responses | Ergonomic responses |
|
Seeing fine detail |
Pressure on manufacturers |
Magnification |
Oblique lighting Colour contrast |
| Control of fine movement |
Intuitive | Finer instruments | Design for the external precision grip Stiffness standard of 0.6-0.9 N |
| Steadied posture |
Seating needed | Limited attention to seating | Modern chair design Height adjustment seat-pad design |
| New manual techniques | Trial-and-error |
— |
Analysis of handgrip and movement |
| Inadequate mental models of anatomy |
Experience | — | — |
| Habitual methods of work |
Experience, limited analysis | — | Skills analysis |
Today the continuing developments in endosurgery are driven harder and faster by several powerful factors: the larger number of patients and surgeons, media, complications, litigation, commercial opportunities, and the perennial surgical drive to improve operative procedures. However, there are constraints, comparable to those of the early phase of microsurgery, which can be summarized in a similar way and are discussed later (see Table 2).
Table 2. Comparing micro- and endo-surgery
|
Type of surgery
|
Principal change from open surgery
|
| Microsurgery | scale |
| Endosurgery | access |
This paper reports a 3-year analysis of applying ergonomics to endosurgery. During the preparation of this paper it became clear that the systems approach, so integral to ergonomics, must be extended in this case to include the engineering properties of tissue and its implications for gripping, dividing, and repairing it, and also to include the experience of surgery itself.
The rest of this paper consists of five sections:
(1) Ergonomics and the systems approach
(2) Constraints of access in endosurgery
(3) Tissue properties and the elements of dissection and repair
(4) Systems integration
(5) Applications and future research.
Ergonomics and the systems approach
Ergonomics is 'the scientific study of people at work, in terms of equipment design, workplace layout, the working environment, safety, productivity, and training'. Ergonomics is based on anatomy, physiology, psychology and engineering, combined in a systems approach.
Systems are the subject of a rich literature 4. A system can be defined as a set of objects or items with links between them. Any type of surgery is a 'socio-technical' system because it includes both relations between people and with technology. It also includes factors in the work environment, the tasks carried out, and intangibles such as information and management.
In a complex system, problems or changes in any one item may have drastic often unexpected effects on other parts of the system. These are studied in Chaos theory 5 and more recently in Complexity theory 6, 7 . The politicians' metaphor for unexpected outcomes is 'it seemed like a good idea at the time'.
One component of surgical systems that needs more study is the gross physical properties of soft tissues and vascular tissues. In endosurgery these must now be handled by much thinner instruments, with less mechanical advantage, less transmitted force, and smaller working ends.
In open surgery the mechanical properties of soft tissue have been taken for granted and ignored. Surgeons did not explicitly analyse how tissues were gripped, and how they were divided. It had always been possible to choose a heavier instrument or use several extra instruments of the same kind to secure tissue, and to alter their locus and direction of approach. However, in endosurgery the present generation of graspers can not grasp thick inflamed tissue securely, such as empyemas of the gall bladder, without tearing them and spilling their contents. Dividing tissue is only possible in arcs centred on the site of the port in the abdominal wall. A different angle of attack can be achieved by moving the port or the tissue (especially rotating the tissue by rotating forceps that are holding it), or using an angled instrument. Setting up tissues, dividing them, and dealing with bleeding all take extra time, during which there is escalation of problems of bleeding, spill, orientation, and arrangement of structures.
(Another system component, care and maintenance of instruments 8, is important and sometimes critical to system performance and outcome, but is not considered further here.)
Constraints of access in endosurgery
The core feature is access through narrow channels fixed in position but not direction, for transmission of sensory information in one direction, and for the usual physical inputs for dissecting and approximating tissue in the opposite direction.
As in the early years of microsurgery, an initial basic constraint, in this case narrow ports fixed in position but not direction, was accompanied by others: models of anatomy and pathology developed in the context of open surgery, incongruous designs of instruments, and techniques needing development. The conceptual leap needed for endosurgery is even bigger than that for microsurgery (Table 2). The constraints are similar in principle, but more numerous, and require a larger number of strategies (see Table 3)
Table 3. Constraints in endosurgery
|
Category
|
Type
|
Effects
|
| General | Use of ports | Fixed positions, limited degrees of freedom (see
below) Narrow calibre Limited number, clashing |
| Visual | Seeing fine detail | Resolution Clarity Focal length |
| Illumination remote, coaxial with vision |
Loss of moulding effect of oblique lighting
Blinding contrast if high glare Low for wide view |
|
|
Monocular camera with fixed pivot |
Some loss of depth perception |
|
| Mechanical | Instruments long, thin | Poor mechanical advantage, impaired grasp Small jaws, tissue damage |
|
|
Dissection remote |
Indirect tissue grasp Less familiar movement Impaired control |
|
Narrow openings |
Difficult removing bulky tissue |
|
| Design of instruments |
Lack of improvement | e.g. pistol grip, causing limited rotatability |
| Technique of dissection |
Inherited from open surgery | Cannot be applied without extra analysis |
| Human capacity |
Lack of adaptation | Techniques based on freer access |
|
Design of systems |
Ignored | Lack of compatability and integration Bad workplace design |
The transition from open surgery to endosurgery requires radically different instruments, techniques, and skills. Patchwork changes to them have worked well for easy cases, but the margin of safety has been smaller. The instruments and techniques of modern open surgery evolved over a century by trial-and-error. Without the luxury of this drawn-out timescale, it becomes necessary to take a less piecemeal and more analytical approach. This means starting from scratch by re-examining the fundamental nature of the tasks performed in surgery in general, and then the special constraints imposed by minimal access surgery.
Constraints on viewing
The first essential for surgery is clarity of view. Structures are defined surgically by the simultaneous processes of mechanical separation, visual separation, and sometimes tactile separation from the camouflaging tissue in which they are embedded. Mechanical separation continues until the structure can be recognized, when it may be further mobilized.
Many factors determine the first moment of recognition for each part of the structure, such as image quality, touch, operator skill and experience, and techniques or tricks such as stents or coloured dyes, but the ability to see tissue detail is crucial. There are two other major differences between the normal field of vision and that in endosurgery (Table 4).
Table 4. Constraints on viewing in Endosurgery
| 1. Clarity 2. Viewing distance = 1/10 open surgery. 3. Lost peripheral vision (60° cf. 150°), incoming instruments, end of a suture |
The viewing distance in endosurgery is much shorter, down to 10 times less. It is like reading a page held next to the eye. The angular width of view is also much less, only 60° through a telescope compared with 150° for both eyes. It is literally tunnel vision.
Loss of peripheral vision hides incoming instruments, structures from which a grasper might have slipped, and the end of a suture. Experience compensates for this only partly.
3-D systems are the subject of energetic current developments and reports. However, some perception of depth is possible with video-viewing systems, and, with experience, operators become more skillful at judging depth. For example, inserting instruments through ports in the correct direction is difficult without binocular vision, but it can become second nature after some weeks by triangulating consciously the intended path in three dimensions. This is done by using information outside the operating cavity, relating the path to at least two other ports centred on the same target area. (This is not possible if the instrument must be threaded around adhesions or other structures, which would be at risk of damage.) When surgeons first start in this field they must begin by viewing each instrument as it is introduced into the abdominal cavity. Of some 16 cues for depth perception, only four or five are lost on a flat screen (Table 5).
Table 5. Cues for depth perception 9 - 11
|
From video monitor
|
Cues lost on monitor
|
| 1. Touch-confirm 2. Gestalt (mental model) 3. Linear perspective 4. Relative size 5. Relative brightness 6. Detail perspective 7. Aerial perspective 8. Interposition/occlusion 9. Shadows 10. Plane height 11. Structure through motion |
1. Binocular disparity (stereopsis) 2. Motion parallax 3. Convergence 4. Accommodation 5. Eye dominance (texture fade) |
Improving clarity gives a disproportionately greater improvement in depth
perception by improving textural gradients and other raw information by
which the operator reconstructs the mental model more accurately. These
are discussed further in Appendix 1.
Mechanical constraints on instruments
There are several mechanical constraints on endo-instruments compared with open surgery (Table 6).
Table 6. Mechanical constraints on instruments
| • thin weak instruments • poor leverage • poor jaw design - grip-oops-slip —> tearing |
These include the thin weaker handles and small joints, which break more easily, despite tissue graspers which have a less mechanical advantage. Jaws grip less well. There is a common sequence of grip-oops-slip grip-oops-slip. There must be changes both in surgical technique and instrument design, based on a re-study of fundamental aspects of tissue grip.
Three other constraints to be considered are new principles for instrument design, operator factors, and system factors. Major manufacturers are seeking increasingly advice on instrument design from surgeons. Advice based on traditional paradigms will continue to fail; a fresh view of the interaction between instruments and tissue is presented later.
Degrees of freedom of movement (DOFs)
This concept is necessary for understanding mechanical constraints. A DOF is the potential for movement in a single independent direction, or a rotation around one axis. In the familiar x, y and z axes there are three possible linear DOFs which are independent of each other. These are sometimes described as translations, or movements which do not include rotation. DOFs also include three rotations, which will be familiar to sailors and pilots, namely pitch, roll, and yaw. A point has three DOFs, because it can be translated (moved) in three independent directions, which are of course usually combined, while rotation has no meaning for a point. A solid object, such as a pencil, has six DOFs, because it can be translated in three directions like a point, and also rotated about three different axes. A straight line has five DOFs, because it has no thickness, and so rolling along its length has no meaning.
DOFs are easy to see and understand if you hold a pencil at eye level (perhaps just an imaginary one) pointing away from you. You can move it from side to side, up and down, and towards and away from yourself, and you can combine these movements in different ways. You can also rotate the pencil about any one of three independent axes; you can twirl it (rolling), waggle it from side to side (yawing), or wiggle it up and down about its centre point (pitching).
If in your imagination you now replace the pencil with a long handled instrument pointing obliquely downwards, in an imaginary port in the wall of an imaginary distended abdomen, and think of the x-y plane shifted so it is now lying onto the skin, you can move it in various ways. You can roll (rotate) it in the line of the z axis, waggle it from side to side pivoted on a point in the y axis, and wiggle it up and down about the x axis. You can also move the instrument in and out (translation in the z axis), but there is no movement possible in the x or y axes unless the site of the port can be moved a little by stretching the skin or by tearing the opening in the skin. For such an instrument, typical of endosurgery, there are only four DOFs of movement available.
Other terms for translations will be more familiar to amateur video buffs. Z movement is also 'zoom in/out', yaw is 'pan left/right', and pitch is 'tilt up/down'. These refer to the image rather than the manipulating hand, which helps explain the confusion of the camera operator when the operator says 'move left' rather than 'pan left'. We have described this elsewhere" as 'first order paradoxical movement'.
This also explains some of the severe frustration of surgeons early in their laparoscopic career. They are used to moving instruments freely over the body and in large cavities created by long incisions and retraction of tissues. For their own body they have two DOFs for where they stand, six DOFs for the position or bending of their trunk, one or two at the scapulo-thoracic joint, three rotations at the shoulder, one at the elbow and one in the forearm, and two at the wrist. There is a complex mobility from several types of protraction and retraction by the precision grip of the hand, as well as rotation of instruments within the fingertips. These probably constitute two DOFs at each of five metacarpophalangeal joints and one DOF for each of nine interphalangeal joints, giving a total of 19 for the hand, and a total of 32 DOFs at the fingertips, or 36 if an extra three DOFs are allowed for positions of an object within a flat grip of the fingertips (two rotations and two translations; open to argument).
How many DOFs are there in placing a needle in the jaws of a needleholder? Simple analysis shows there are four. (Readers may like to work this out for themselves before reading further.) The four degrees are: distance along the jaws, distance along the needle, rotation of the needle about the axis of that part of the needle in the jaws, and obliquity of the needle. All surgeons are familiar with the additional little adjustments of needle position when suturing a deep difficult structure.
This does not finish the analysis of DOFs, as the range of movement varies greatly from one situation to another. As an example, pronation and supination of the forearm can rotate an instrument almost two right angles, which also varies with the agility of the surgeon. This can be increased further if the handle design allows rotation to be controlled by movements within the hand, an important factor discussed later in more detail. Such rotation is not possible within ring-handled instruments if the thumb and fingers are placed too far into the rings. Other limits to the range of motion within a DOF are instrument clash, collision with tissues (increased with loss of pneumoperitoneum), and restriction of the range of movements of the surgeon. On the other hand the effective range of a DOF can be increased by stretching, depending on the elasticity of the tissue and how it is moved, perhaps helped by an assistant. Knee surgeons can do this by re-entering the joint capsule at a more favourable site whilst still using the same skin incision.
There is a further complexity introduced by angled components, whether a slight curve at the end of a needleholder (very effective for knot tying) or an angled light beam or 'reticulated' (hinged) instrument, or a flexible one. To a greater extent angular movements also become ones of translation. With multiple elements linked together in an articulated system, the range of positions for positioning a working end is increased.
There are other respects in which six DOFs will not be enough for endosurgical manoeuvres. Access imposes additional needs. For example, access around the side of a structure, or behind it, needs an extra 'wrist' in the instrument, like the second elbow joint one would like to have to reach a bedside lamp behind one's head. A special starting point may be needed for the passage of semicircular needles along an arc rather than a straight line, or for retraction or other manipulation around corners. Some manoeuvres will not be possible, for example passing a needle through a particular curved path without stretching or damaging the tissue.
The final limitation of DOFs is the capacity of the surgeon to visualize the work-space in the patient's body cavity and the movements of structures and instruments within it. It is not normal for humans to move in Cartesian coordinates or analyse their movements as separate elements in each of three dimensions. The animal brain and body are used to working in curves based around hinges at several joints simultaneously. If the arm on a joint is sufficiently long, a small range of movement is near enough to a straight line rather than part of an arc. Being able to work comfortably with these constraints is important for the assistants as well as the operator, whether in moving the camera or various instruments. The relevance of DOFs to endosurgery is summarized in Table 7.
Table 7. Degrees of freedom
|
Object
|
No. of DOFS
|
|
A free object |
6 >36 * 4 |
* These comprise 2 for foot positions, 1 for crouching, 2 for trunk rotation and bending, 1 for scapulothoracic joint, 3 for shoulder, 1 for elbow, 1 for pronation-supination, 2 for wrist, and 17 finger joints of which 5 have an extra degree of adduction-abduction or circumduction.
Port placement, patient posture
The constraints imposed by limited access and limited DOFs make it particularly important to place ports correctly. Experience shows that, as for work in general, there is no one accepted `best way' for placing ports, or indeed for arranging the posture of the patient. For laparoscopic cholecystectomy the French position has the operator between the legs, the Reddick technique has the patient supine with the operator on the left side of the patient, while a current technique used by Graber has the surgeon on the right side of the patient, with one assistant and two ports close together in the right upper quadrant and a third port for the telescope, as usual, at the umbilicus.
Port placement can be determined in different ways: by experience, habit, guesswork, by testing the position with a needle, or by analysing the processes used in dissection which are described later. If the best directions for grasping, retracting, and dividing tissue are then determined, these lines are projected from the target site to the inside surface of the abdominal wall, and then to the outside. This then indicates the site for the port. There must be enough length of instrument clear past the inner end of the port to clear the hinge joint so as to allow free opening of the jaws or blades of various instruments. Security against port displacement is often needed, whether by a coarse screw, suturing, or expanding flanges.
Tissue properties and the elements of dissection and repair
Tissues vary in their consistency and strength on a spectrum from bony-hard to jelly-like. Surgeons need an expanded range of adjectives, nouns, and measures to describe such properties.
Such properties also vary in different directions and under different physical and chemical influences. When inflammation or scarring blurs the demarcation between structures, both sharp and blunt dissection become less predictable, making damage to the structures on each side of the line of dissection more likely.
Dissection is so familiar from open surgery that it is taken for granted. In open surgery with free access and a wide view, there is little problem in positioning forceps or the fingers to grasp tissue by a fine edge or in bulk, or to re-grasp it. Tissue can be steadied widely by several fingers in different position and from different directions, rotated and moved widely, and divided in large sweeps in clear view. If bleeding occurs, bleeding points are generally exposed quickly by retraction from several directions and by mopping or suction, staunched by direct or indirect pressure such as tensing over the fingers, and then diathermized or clamped, tied, or oversewn. Under the constraints of endosurgery, such actions are limited in number, direction, extent, rate, and force. Such processes as exposure, application of pressure to blood vessels, suction, orientation of tissues, suction, and diathermy must be reexamined to determine their essential details and how these may be modified. Some of the conclusions that result might be reapplied to open surgery to improve it, as well as to endosurgery to make it possible. The elements of dissection and repair are summarized in Table 8.
Table 8. Elements of dissection & repair
• exposure
• stabilization = tissue grip + pull if loose
• division
• repair
Exposure is defined as developing a suitable space for seeing and handling target structures. This space has 6 definable components 12 aligned in various directions from the target of dissection to the body surface:
- Volume occupied by instruments
- Volume described by movement of instruments and hands, in open surgery
- Volume occupied by hands at rest
- Volume occupied by movement of hands
- Conoid(s) of vision (two if binocular)
- Conoid(s) of illumination (point of conoid down in open surgery, up in endosurgery).
Each of these can be described in more detail and quantified, for example the track of a needle through space as well as through tissue, the clearance needed by a tissue stapler in a narrow pelvis, and straight-line access for lighting and vision.
Heuristics: tissue division and tissue grip
Once tissue is exposed, the processes of grasp and division follow a series of heuristics (rules of thumb from experience - from the same root as Eureka and the legend of Archimedes' principle). Tissue pull or grip and tissue division are taken for granted in open surgery. For more effective dissection in endosurgery, the mechanics of these processes must be examined anew. If the heuristics are incorrect or unknown to the operator, dissection is inefficient. In a logic based on sequence, grip should be examined before dissection or division of tissues, but as this requires a preliminary analysis of the mechanics of stability, it will be easier for the reader to consider the more easily considered phenomenon of tissue division first. Here is a series of heuristics for optimizing dissection in general.
(1)Homogeneous tissue is divided most readily at right angles to lines of tension.
(2) Tearing of structures which are not homogeneous tends
to follow lines or planes of cleavage (lines or planes of decreased tissue
strength).
(3)The line of tissue division is more likely to follow planes or lines of tissue cleavage the more slowly it is divided. (This allows short fibres crossing the plane enough time to tear before tension is taken up by the next group of fibres, rather than the structures on either side tearing. This can be demonstrated by tearing thin card into two layers slowly, and then speeding up). Contrariwise, a quick thrust is more likely than slow piercing to impale tissue such as tough skin edge in a chosen configuration such as eversion if it is not held firmly enough to avoid distortion during the passage of a suture needle.
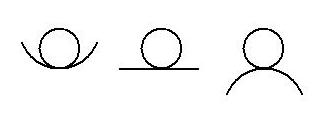
(4) 'Funnelling', as in pouring liquid, is a concept that can be applied to solid structures. It is the guiding of movement into a particular direction by constraints, and is equivalent to the stable mode of the three modes of equilibrium (Figure 1).
(5) Funnelling helps control the steadiness and accuracy of hand movement. It also determines the direction along which the tissue tears. (Funnelling is described further below.)
(6) To make soft tissue tense requires as many points of traction as there are tongues of tissue, or repeated application to successive points as the incision progresses.
(Such tongues can be defined mathematically according to the potentially convex and concave curvatures of their edge, thus explaining the frustrations in trying to divide floppy tissue under close scrutiny but not its contained vessels.)
(7) For exposure (and dissection), overlying tissue must be held back in bulk or else have any laxity of the surface tensed in drawing it away, which may include tensing multiple tongues of tissue.
Scissors cut tissue by a mechanism that must be considered separately (Appendix 2). Soft poorly elastic tissue such as liver can be divided by 'finger-fracture' 14, 15 , leaving vascular and biliary channels intact for separate ligation or diathermy and division. Omental adhesions can also be thinned of fatty tissue in this way.
For endosurgical dissection these heuristics must be refined to take into account the constraints discussed earlier, and their implications for dissecting and instrument design acted on.
Stability and funnelling
A second group of principles for dissection is guiding or coaxing actions along one course rather than another. In mechanics there are considered to be three types of equilibrium, referred to as stable, neutral, and unstable. These can be illustrated by the three ways a cone can rest on a horizontal plane (on its base, its side, or its point) or the three surfaces on which a sphere may rest (in a hollow, on a flat horizontal plane, or on a smooth convexity) (Figure 1).
Figure 1 Three modes of equilibrium
 |
|
Stable |
Neutral
|
Unstable
|
Stable equilibrium is similar to using a funnel to direct liquid into a narrow opening, or a ruler to draw a straight line, or designing a tapered peg to fit more easily into a chamfered hole (one which has been bevelled to guide the peg better). 'Funnelling' is the arrangement of work so that a range of movements are guided into a particular pattern, despite some variation in the input. A funnel typically controls spill. A funnelled movement occurs when cutting into the linea alba if the two rectus muscles create a dip between them so the belly of the blade runs more easily in the groove. It is easiest to free a rib from the external intercostal muscle by rasping forward into the acute angle on its upper edge, and backwards on its lower edge, a principle illustrated by A. K. Henry in relation to posterior attachments of the femur 16. He also describes dividing with scissors between the two heads of gastrocnemius like ripping a sleeve to open it up. In this case the partly opened scissors also have a funnelling effect, similar to two forked sticks pressed in a stable way, each into the cleft of the other.
Such funnelling guidance is usually followed better by a blunt instrument. It can be spoiled by a sharp edge which catches into the tissue on either side of the funnelling and so loses its direction, or by excessive force or speed, or by using destructive energy such as diathermy.
As an example of these principles, consider the common accident of perforating the gall bladder while separating it from the liver bed, often during the middle of this dissection. A reliable way of avoiding this would be welcome. The relevant factors involved are listed (Table 9).
Table 9. Factors
in perforating the gall bladder
|
Under immediate control of operator
|
Under operator's direct control in the longer
term
|
Factors not under operator's direct control
|
| View of 'dotted line' of dissection |
Operator experience, skill Ability to recognize tissue boundaries | Patient-related: consistency and configuration of tissue structures |
| Tension on gall bladder and liver, to widen the 'dotted line' and improve separation | Personal stock of heuristics for exposure, preparation of tissues, (e.g. infiltration, intubation of structures), more accurate control of instruments | Equipment available: design for grasping (see below) |
| Emptying gall bladder Grasping of gall bladder Retraction of liver Speed of dissection (in cm or mm/s) Instructions to assistant |
Skill of the assistant Organization of team, quality and care of equipment |
Methods of grasping tissue: implications for instrument design
One of the fundamental questions raised by such analysis is 'how is tissue gripped to stabilize it?'. Pull or grip for stabilizing or moving tissue can be considered in four modes: a single applied force, embrace (without compression or squeezing), a pair of applied opposing forces, or attraction such as suction, which is of course atmospheric push (Table 10).
Table 10. Tissue grip and stabilization
|
Stabilizing force
|
Example
|
|
(1) Single force |
Flat retractor under liver Single skin hook |
| (2) Embrace or encirclement |
Encircling forceps, tape |
| (3) Paired opposing forces - friction - Indentation / transfixion |
Gripping forceps |
| (4) Suction or other attraction No serious damage should occur |
Vacuum extraction during labour |
(1) A single force may have two or three properties:
• it is applied in the desired direction of pull,
• on a flat surface, such as liver, say, there must be enough friction
to stop it sliding off, and/or
• there must be a concavity or negative curvature, similar to that
in the physical model of stable equilibrium. This also includes partial
transfixion by a sharp point or local indentation. Unfortunately it can
lead to laceration of a structure such as liver.
(2) Embrace or encirclement. Littlewood's, Babcock's, and Allis forceps may be quite atraumatic as long as they close completely around the structure without squeezing it.
(3) If a single force or encirclement can not be applied in one of the above ways, it is necessary to apply paired opposing forces. These also need to have one of two properties:
• enough friction,
• enough compression, indentation, or other deformation, without
causing damage to tissue, especially leakage from a cavity or tube.
In other words, pull can be applied to a flat surface which does not slip, or to a hollowed surface (including for example, a tissue hook). The direction of pull is critical, and the correct direction may not be available through a port. If that is so, the tissue needs to be encircled, or gripped. Encirclement is secure, and atraumatic, but requires a (potential or actual) hinged pair of ends sufficiently curved to encircle the structure, possibly too big to pass through a port, or an encircling (flexible) tie or tape, or transfixion. (One analogy is given by obstetric forceps pulling on the foetal head - there must be many others.) Otherwise a paired grip is necessary. Methods of grip applied to different tissues are summarized in Table 11.
Table 11. Tissues and methods of grip
|
Tissue
|
Properties
|
Holding method
|
| Inelastic tissue with firm attachment
to body |
Body weight acts as one of the two anchors | None needed except for drawing open the line of incision |
| Skin edge | Tethered, e.g. umbilicus | Firmer toothed forceps Evert with Moynihan forceps |
| Subcutaneous fat in obese patient |
Flops, obscuring line of sight | Deep narrow non-fenestrated retractors, may be self-retaining |
| Mucosa | Fragile, rugose |
Blunt gentle forceps, or none locally Stay sutures Spreading open with downward pressure |
| Hollow viscus | Slithery, elastic Fragile attachments
Wall may be damaged |
Forceps, fingers gripping forceps, fingers
encircling Grippable tube inside (e.g. n.g. tube in stomach) |
| Solid viscus | Fragile Non-elastic |
Blunt and wide Parallel to surface |
|
Gall bladder, healthy wall, not distended |
Floppy healthy Tolerant |
Several options - toothed, crushing ± emptying |
| Gall bladder, thickened | Slithery, thick, fragile |
Embracing but not traumatizing jaws (yet
to be designed - very large Babcock) internal balloon e.g. Foley catheter |
|
Greater omentum, other non-surface loose fatty tissue |
|
(Fingers ±gauze) |
| Plane of division obscure | Atraumatic / toothed forceps Retractors Gravity (tilting, up to 180° rotation of body e.g. access to oesophagus) |
|
| Vascular tissue | Fragile vessels may bleed so tissue is obscured | Mechanical, thermal, laser |
| General | Consistency, strength | Retract/squeeze/pierce/embrace/suck |
Timing and time taken
Good timing in significantly resisted movement has been defined elsewhere 18 as that rate of application of force which maximizes the transfer of energy through part of a system. For dissection, a new definition is needed for good timing because of the particular nature of the task. Accuracy is the aim, and not the quick transfer of a large amount of energy. In this case, good timing is that rate of operation that allows the operator to manipulate tissue states and to recognize the changes effected, with minimum error and maximum control, and not at any particular speed, whatever its other advantages and problems may be.
Unlike skilled 'ballistic' movements 19,20 repeated checking of successive small movements of this kind have a much slower cycle time, with a minimum of 80 msec for each of perception, mental processing, and controlled movement 21. In some surgery (microvascular and neurosurgery) and with critical scarred structures, each element of movement may take many seconds instead of a fraction of a second, so that feedback is in much smaller chunks and movements altered at a much smaller cost in damage to structures.
During endosurgery, timing takes on an extra meaning because of delays owing to limited access. Bleeding from floppy vascular tissue is a particular problem because it obscures the tissue view to a greater extent than during naked eye viewing, and is more difficult and time-consuming to control when it occurs. Suction interferes with pneumoperitoneum and gauze swabs, if used, take much longer to apply and remove. Dry dissection, by whatever means, is an investment worth a high premium of effort. Haemostatic clips take many times longer to apply to bleeding points than artery forceps, while problems of visibility escalate at a much faster rate. Unlike open surgery where an extra instrument does not need an extra incision, each additional instrument would need an extra port and an extra few minutes just when bleeding might be taking place. Prevention and control of bleeding during endosurgery is a major consideration, and its finely detailed analysis a matter of importance.
Apposition of tissue
Closing tissue gaps by staples or sutures is the everyday task of most surgeons, and is done intuitively on the basis of experience and the particular circumstances, e.g. type of tissue, properties and their alteration, and tension. To some extent the closure of gaps can be modelled by studying two tissue properties:
(1) plastic and elastic deformation, using finite element analysis, and
(2) spacing, setting back, and tension of the sutures or staples, and the allowable size of the gaps that are left.
How small is a hole? Tissue gaps have a lower limit below which they do not need to be closed to achieve integrity. This lower limit depends on:
• pressures on the two sides of the gap,
• viscosity or consistency of the material which may leak or herniate
(these factors vary with time, whether for clotting or healing and scarring),
and
• inverting closure technique, which acts as a double flap valve.
The endosurgery system has three main groups of components: physical, human, and intangible components such as information and management. As in other systems, if they are not well designed specifically to work together the results are delays, errors, and waste.
Problems of standards
Some incompatibilities between equipment are deliberate, for example to make it impossible to connect a nitrous oxide supply to an oxygen inlet, or a low voltage device to a high voltage source. Others hinder the operation, for example different connectors for diathermy instruments.
Most incompatibilities are due to lack of planning. They may be merely an inconvenience, or a danger. They are not common in mature industries, where national and international standards have been developed. In the case of an immature field, such as the manufacture of endosurgical equipment, the situation is otherwise. Competition between big manufacturers of surgical instruments stimulates the quickest possible development of new and better designs. It allows small start-up companies to enter the market if they have a good product which may then be taken up widely. Its drawback is the lack of compatibility and integration when systems are assembled from components from different manufacturers.
These problems might be avoidable by buying from only one manufacturer but at the cost of restricted choice. Another company may have, say, a better needleholder or a better tissue grasper or bipolar diathermy forceps. (It takes months or years to develop, test, and produce new instruments, and a heavy investment of money. When mistakes occur or companies misjudge the market, their share price tumbles. This happened in 1993 as a reaction to the euphoria of the first wave of laparoscopic surgery, as problems were reported and complications became more common.) Enthusiasm by one leading manufacturer for the 'Operating Room for the Future' has not yet led manufacturers into designing integrated systems, nor has it led to common standards with other manufacturers so that equipment of different brands would produce a smoothly functioning system.
Human-machine interface problems
Humans and equipment are often incompatible when the engineering design of equipment ignores human dimensions, human performance, and human limitations. Examples are:
• video monitors above the eye height of the operator instead of
15 to 30° below it,
• confusing controls,
• instrument handles <sup>22</sup> with a pistol-style
grip which limits rotation to that of the forearm, instead of a co-axial
grip that allows rotation within the hand,
• reflected glare from shiny instruments,
• excessive friction from ports, impairing both tactile feedback
and fine control of instruments.
Video carts exemplify several of these problems. Design and layout of controls and readouts on insufflators, light sources, and video monitors ignore detailed information on design, available in standard industrial guidelines which have been applied to computers, industrial control systems, the cockpits of aircraft and spacecraft, and many or most other manufactures. They are not `user-friendly'. These controls and readouts also differ in style from one manufacturer to another. (A huge literature has developed in this area in the past 15 years. See, for example Card et al 21, Helander 23, Department of Defense 24 ).
Connections have to be made to awkwardly-placed sockets and create a spaghetti-maze of wiring that need time-consuming rearrangement with any alteration in the equipment being used. Just as VHS video took some years to displace the Sony Beta standard completely, so many surgeons will have some years of working with 'orphan' systems components until generally accepted standards emerge.
Applications and future research
A detailed ergonomic analysis of the tasks of endosurgery will take significant resources and time. It will not only support the tasks of the surgical team for advanced procedures, but also to make the average cholecystectomy safer, and the difficult laparoscopic cholecystectomy both feasible and less time-consuming. The matter of tissue-grasp has been analysed, if only in outline. Some other areas are considered now.
Handle design for grip and rotatability
A surgical instrument may need to be rotated along its long axis for different purposes; changing orientation for gripping or cutting a structure, applying clips or staples, or suturing. Such rotation can be achieved in different ways (Table 12).
Table 12. Methods of rotating surgical instruments
|
Type of movement
|
Example
|
| Body and shoulder movement | Gross movement of instruments, tissue |
| Forearm pronation/supination (the commonest rolling
action in open surgery) |
Suturing |
|
Rotation in hand and fingers |
Finer suturing |
| Twirling within the fingertips |
Microsurgery |
In this context, instrument handles may be considered in several families, both in general surgery (Table 13) and endosurgery (Table 14).
Table 13. Rotatability of general surgical instruments
|
Pre-endosurgery examples
|
Ring-handled
|
Non-ring-handled
|
| Co-axial | Artery forceps Weck disposable hemoclip applier Colonoscopy biopsy forceps (one thumb ring, two finger rings) |
Mathews needleholder Various staplers |
| Pistol grip | Sigmoidoscopy forceps ENT instruments |
Various staplers |
| Cylindrical | Not relevant | Microsurgical needleholders and tissue forceps e.g. Vickers |
Table 14 Rotatability of endosurgical instruments
|
Endosurgery examples
|
Ring-handled
|
Non ring-handled
|
| Co-axial | None | Ethicon, VMueller and Jarrett needleholders |
| Pistol grip, with or without shaft rotated by thumbwheel* | Graspers, scissors, clip and staple appliers, some
early needleholders |
GIA staplers |
| Cylindrical | Not relevant |
Szabo-Berci lap NH Vickers microsurgical NH |
* Typically these thumbwheels were neither placed in the natural line of movement of the tip of the digit, nor scalloped in a suitable shape and size, nor of appropriate rotational stiffness. This has changed recently.
The common design of artery forceps, with two ring-ended handles in line with the shaft, can be described as 'co-axial'. Such an instrument is in line with the forearm. When the forearm is pronated or supinated, the instrument is rotated along its long axis, for tasks such as suturing, and for positioning the working end to cut or grip in the desired direction. Such instruments can be used with the tips of the fingers barely through the rings so that they are easy to disengage. The elbows generally are close to the body and steadied against it, or against the patient. Instruments can be picked up and put down without the rings catching on the fingers. Instruments such as ring-handled tissue forceps can be applied and removed quickly, and may remain in the wound but out of the way of the dissection. (Inexperienced assistants often find it an effort to let go of a haemostat because their fingers are in too far.) Such instruments can be rotated within the hand by several different manoeuvres, such as protraction and retraction of the thumb alternating with the fingers, or flipping between base and tips of fingers and thumb.
By contrast, the pistol grip for ring-handled instruments was designed for simple snipping tasks along the line of sight in an early auroscope or sigmoidoscope, which is not often necessary or even appropriate now. Rotation of the forearm is either at a significant angle to the line of the instrument, or at a distance from it. Rotation of the instrument is no longer possible over the same range and with the same control.
The most finely controlled rotation is within the tips of the thumb, erg_lapsurg_1995, and middle finger. In microsurgery, the closed handles (actually 'fingles') form a cylinder that can be twirled within the fingertips and supported in the cleft of the thumb while the hand is steadied to control tremor 2, 3 . A similar principle has been applied, using thicker handles, in the Szabo-Berci laparoscopic needleholder, though without support in the thumb cleft. (The handles have to be closed nearer their ends than the joint to apply sufficient force comfortably to close.)
The Jarrett needleholder imitates the older Mathews needleholder, with curved handles fitting within the palm. Lacking a pommel, the curvature encourages the handles to slide up so the thumb and fingers have less mechanical advantage in squeezing them together. Newer designs, such as the VMueller and Ethicon laparoscopic needleholders, have straighter handles so that when closed their shape is closer to a rectangular box. These two designs differ in design of handle texture and ratchet release trigger.
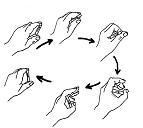
Simple experiments with rectangular boxes show that they can be flip-rotated repeatedly between the base and tips of fingers and thumb, especially if the width of the box equals the length of the slightly closed palm, which is also about the length of the fingers and thumb (Figure 2).
Two rounded edges are flipped instead of twirling the cylindrical mass of the closed handles in the fingertips.
Further refinements of the ratchet mechanism and the surface of the handles still need to be developed 22. This may almost give an ideal needleholder. However, previous experience shows that ergonomic design of a needleholder25 may not mean wide adoption and use. The basic weakness of applying ergonomics in such situations, even when the logic of design appears to be correct, seems to be 'habit is more powerful than logic'.
Tactile feedback
Where dissection is carried out by touch its importance is obvious but its mechanism is rarely discussed. Sir Hugh Devine 26 , an outstanding operator of his generation, was able to describe the use of his own special design of instruments in the peritoneal cavity in these words:
After prolonged use of these scissors - always of exactly the same weight - I have been able to develop with them a sense of touch that enables me to recognize with the tips of the scissors the slightest difference of tissue density, and therefore to identify blood vessels and other structures by the feel of them'.
In endosurgery, such delicate sense of touch largely is lost because of friction between instruments and ports, especially the rubber seals on them, and friction in the transmission of handle movements. Some surgeons seem to feel that no tactile feedback at all is possible, but this is far from true. In hernia repair the bony consistency of the pubis is an obvious landmark. In putting tension on tissue it is clearly possible to feel the transmitted tension through the hands as well as the feedback from seeing it on the video monitor.
The range of forces experienced is from several tens of grams weight to several kilograms 27 (see Appendix 3), from the weight of a mosquito forceps (about 20 g) to the push needed to insert a trochar, between 7 and 14 Ibs weight 28 or about 30 to 70 N.
The challenge to surgical instrument makers is to minimize friction and instrument weight so that there is minimum dilution of tactile feedback and 'touch' to the operator, and maximum opportunity to 'feel' the tissue, even with long intervening instruments. The assistant with only a coarse sense of touch is liable to tear liver with a retractor or repeatedly pull grasping forceps off the gall bladder.
Needle grip by needleholders
Compared with those used in open surgery, laparoscopic needleholders at first did not hold needles firmly. Security of grip by needleholders can be measured easily by pressing the needle onto a kitchen scale, or a more sophisticated push-pull gauge, until the needle twists, when the reading on the scale is noted 29. More sophisticated measurements on laparoscopic needleholders 30 have shown a wide variation between good and bad instruments.
Our observations and analysis suggest a useful role for ergonomics and a systems approach in endosurgery. The problem is not only multi-disciplinary, but inter-disciplinary. It is uncommon for surgeons to have a strong engineering background, and one which includes ergonomics. Engineers, even those immersed in designing medical devices, can not have the deep appreciation of surgeons for the subtle properties of tissues and what is likely to work in a practical situation. It will need strenuous, time-consuming, and costly efforts to bridge this gap.
Future areas for research include: fundamental aspects of dissection, including the operating space and tissue grasp, ergonomic task analysis and design, and systems design and integration.
Surgeons should take a stronger initiative to lead these efforts, or
progress will be slow. If a new view of operating systems and equipment
is successful, it will make the tasks of surgeons and others safer and
with better outcomes. The biggest winners will be patients.
References
1. Menz W, Buess G. Potential applications of mlcrosystems engineering
in minimal invasive surgery, in surgery. Endoscopic Surgery and Allied
Technologies 1993; 3: 171-80.
2. Patkin M. Ergonomics and the operating microscope. Advances in Ophthalmology
1978a, 37: 53-63.
3 Patkin M. Selection and care of microsurgical instruments. Advances
in Ophthalmology 1978b; 37: 23-33.
4 Checkland P. Systems Thinking, Systems Practice. 2nd edn. New York:
Wiley, 1986: 1-12.
5 Gleick J. Chaos - Making a New Science. UK: Cardinal, 1988: 303-17.
6 Lewin R. Complexity-Life at the Edge of Chaos. London: Dent, 1993:10-21.
7 Waldrop MM. Complexity - the Emerging Science at the Edge of Order and
Chaos. UK: Viking, 1993: 11-12.
8 Patkin M. Buying and caring for surgical instruments. In: MIMS Hospital
and Equipment Supply Directory. Sydney: IMS, 1994. xxxiii-xxxxi.
9 Murray J. Visual cues for depth perception, internet newsgroup posting.
Comp Human-factors 5518, 26 Sep 1993.
Message ID: 2859nllNNbsh@srvrl.engin.umich.edu >.10 Kaufman L. Sight
and Mind: Introduction to Visual Perception. Oxford, 1974. Cited in Murray".
11 Wickens C. Engineering Psychology and Human Performance. College, USA:
Harper Collins, 1992. Cited in Murray.
12 Patkin M, Isabel L. Ergonomics and laparoscopic general surgery. In:
Graber JN, Schultz LS, Pietrafitta JJ, Hickock DE, eds. Laparoscopic Abdominal
Surgery. New York: McGraw-Hill, 1993: 83-8.
13 Patkin M. Ergonomic aspects of surgical dexterity. Med J Aust 1967;2:775-7.
14 Lin TY. A simplified technique for hepatic resection: the crush method.
Ann Surg 1974; 180: 285-90.
15 Balasegaram M. Hepatic surgery - present and future. Ann RCS Eng 1970;
47:139-58.
16 Henry AK. Extensile Exposure. 2nd edn. Edinburgh: Churchill Livingstone,
1975: 3, 4-5, 260.
17 Mossel WP, Roosen CPG. Friction and the skin. In: Robertson SA, ed.
Contemporary Ergonomics 1994. Proceedings Annual Conference Ergonomics
Society. London: Taylor & Francis, 1994:353-8.
18 Patkin M, Gormley J. Skill, excess effort and strain. In: Kumashiro
M, Megaw ED, eds. Towards Human Work. Solutions to Problems in Occupational
Health and Safety. London: Taylor & Francis, 1991: 145-50.
19 Glencross DJ. The control of skilled movement. Psychol Bull 1977; 84:
14-29.
20 Patkin M. Ergonomics for surgeons. In: Burnett W, ed. Clinical Science
for Surgeons. Sydney: Butterworth, 1981: 577-80.
21 Card SK, Moran T, Newell A. The Psychology of Human-computer Interaction.
New Jersey: Erlbaum, 1983: 23-97.
22 Patkin M. A check-list for handle design. In: Proceedings of the 1985
Victorian Occupational Health and Safety Convention, 1985:307-14.
23 Helander M, ed. Handbook of Human-computer Interaction. Amsterdam:
North-Holland, 1990.
24 Department of Defense (1992) Military specification for human engineering
requirements for military systems, equipment and facilities (dcc # MIL-STD-1472D).
United States Government Document.
25 Patkin M. Ergonomic design of a needleholder. Med J Aust 1969;2:490-3.
26 Devine H. Surgery of the Alimentary Tract. Bristol: Wright, 1940: 351-2.
27 Patkin M. The ergonomics of hand function and handle design. In: Eighth
Annual Ira Symposium, on New Vistas in Management and Quality of Work
Life, Ira Memorial Foundation, Tel Aviv, 1980.
28 Corson SL et al. Measurement of the force necessary for laparoscopic
trocar entry. J Reprod Med 1989; 34: 282-4.
29 Patkin M. Surgical instruments and effort, referring especially to
ratchets and needle sharpness. Med J Aust 1970; 1: 225-6. .
30 Cartmill JA, Graber JN, Schultz LS, Hickok DF, Patkin M, Isabel L.
Ergonomics and Needle Holding Ability of Laparoscopic Needle Holders.
Poster Display, SAGES Conference (1993), Phoenix, Arizona
Appendix 1 additional notes on depth perception
When looking at a flat screen instead of the open area of a surgical procedure, there is loss of four cues necessary for perception of distance or depth. These are stereopsis (the difference between the two retinal images), convergence (as the eyes turn to or away from each other), and accommodation (as the lens curvature is altered by the ciliary muscle to focus the retinal image according to distance and motion parallax, as the surgeon moves his/her head from side to side to estimate relative distance of overlapping objects. This still leaves half a dozen other less effective cues including mental models of the anatomy, relative size, relative illumination, textural gradients, occlusion, relative movement of structures, and 'touch-confirm' (Szabo, personal communication 1993). One expression of frustration at the loss of depth perception is the familiar sight of operator or assistants uselessly trying to look round the edge of the monitor to be able to see round the structure being dealt with at the time. (It is easy to look over, around, or under an object using an angled telescope, but by moving the laparoscope and its field of view slightly, and not the head of the viewer.)
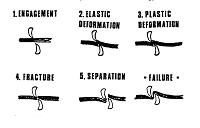
Appendix 2. How scissors cut (Figure 3)
Scissors cut by a combination of gripping, squeezing, and tearing. Their mechanism depends on two blades which are generally hollowed out in two directions; along their length, and from edge to back. The hollowing extends past the screw joint to a raised area which is called the half-moon, shoulder or rise. When the screw is sufficiently tight, the shape of the curves ensures that the two sharp edges grind against one another, so that any tissue between them is crushed to nothing. Angled-on-flat and curved-on-flat scissors achieve a similar effect through slightly different bends or curves on the two blades. In the case of some very slippery material or object, it may slide away from the crossed cutting edges as they are closed. For that reason, some scissors are serrated.
The action of cutting by scissors can be described in 5 stages: engagement, elastic deformation, plastic deformation, fracture, and separation.
If the screw joint is loose, elastic tissue can slip through the gap before the elastic limit is reached. The best test material is glove rubber, or condom rubber for very fine scissors. The two handles must be closed with no lateral pressure. Right-handed scissors with a loose screw can be made to cut by pushing one handle with the right thumb and pulling the other with the fingers. If used in the left hand, the left thumb must pull and the fingers must push. These tricks do not operate if there are extra joints, as in laparoscopic scissors, when successful cutting depends on the integrity of the blade shape, edge, and joint.
Appendix 3. Range of forces exerted in surgical dissection
As well as adjectives it is useful to put numbers onto stiffness, resistance. or forces exerted by the operator. It is necessary to become used to thinking in terms of the relevant units of measurement.
A Newton is the force that accelerates a mass of 1 kg by 1 m,, s. each second. Gravity, which accelerates that same mass 9.8 m,' sec=. exerts a force of 1 kg weight. A Newton is about one-tenth of a kg weight, or about 100 g weight, or the weight of the small English apple which fell on the head of Sir Isaac Newton. An olive pip averages about 1 cm in each dimension, and just sinks in gin which is almost isogravic with water. A ball-point pen has the approximate dimensions of 10 olive pips laid end to end, and is lighter or heavier than water depending on whether it is made up of air and plastic or air and metal. A litre of watery liquid (milk, juice) weighs little more than 1 kg.
An easily remembered scale of everyday weights is as shown in Table 15.
Table 15 Spectrum of common range of applied force and tactile sense
|
Weight
|
Everyday equivalent
|
Force
|
| 1 g weight | Olive pip | 0.01 N |
| 10 g weight | Pen | 0.1 N |
| 100 g weight | Small apple | 1 N |
| 1000 g weight | Litre | 1O N |
| 10 kg | 2-year old child | 100 N |
The typical stiffness of artery forceps (the force to close the first step on the ratchet, applied at the fingertip rings) is 10 to 20 N, and for mosquito forceps, half that force. The peak force needed to push one brand of reusable trochar through the wall of a distended abdomen is typically 66 N (s.d. = 29) compared with 32 N (s.d. = 24)23. The force applied to the tip of a needle to twist it in the jaws of a poorly gripping needleholder is typically 2 N, compared with five or ten times that for a securely gripping needleholder (reference 24 and personal observations). This provides a language by which surgeons and engineers can communicate with one another.
-o0o-Introduction
Ergonomics and the systems
approach
Constraints of access in
endosurgery
Tissue properties and the
elements of dissection and repair
Methods of grasping tissue: implications for
instrument design
Systems integration
Applications and future
research
Conclusion
References
Appendix 1 Additional notes on depth
perception
Appendix 2. How scissors
cut
Appendix 3: Range of forces exerted
in surgical dissection
_______________
J. R. Coll. Surg. Edinb., 40, April 1995, 120-132
This paper was written jointly with my colleague of 10 years at Whyalla. It was published 15 years after I had thought of shredding all my notes on applying ergonomics to microsurgery.
However the same principles apply - a new human-work interface to analyse using ergonomics. The newness is that of yet another type of technology forming a layer between the person and their work.
Publication came about because I sent an informal paper I had written to Sir Alfred Cuschieri. His department of surgery at Dundee had a strong involvement in ergonomics applied to lap surgery, and I thought it might interest his team.
To my delight he asked if it could be published in the JRCSEd of which he happened to be editor at the time. The reply was a very rapid yes!
————
Operative and technology section
Review
Ergonomics, engineering and surgery of endosurgical dissection
M. PATKIN AND L. ISABEL
Department of Surgery, The Whyalla Hospital, South Australia
Expanded version of a paper presented at the Annual Scientific
Meeting of the Royal Australasian College of Surgeons, May 1994, Hobart.
Correspondence to: M. Patkin, Department of Surgery, The Whyalla Hospital,
Whyalla, SA 5600, Australia. mp [at] mpatkin.org
-o0o-