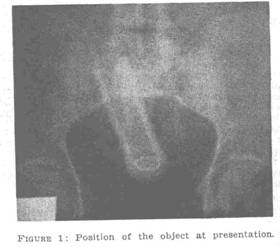
SIR: Avoiding laparotomy to remove an awkward foreign body in the rectum seems worthy of record, as the experience described below may be of help to others. Some time ago (the obscurity is deliberate) I was referred a patient with the history that he had lost something in his rectum a few hours earlier. The patient, a big-built man, had a large electro-mechanical vibrator put in his rectum by his girl friend, as a diversion from their activity at the time. Rectal examination revealed the butt of an elongated object just palpable to the fingertip. Abdominal X-ray examination established the dimensions and attitude of the object (Figure 1).
Under skilful anaesthesia by the partner of the referring doctor, anal dilatation to four fingers was carried out. The object could not be grasped in sponge holders and the traditional use of obstetric forceps (applied to a turnip by others in similar circumstances) seem unpromising. Only when a full dose of relaxant anaesthetic was given to the patient could the object, impalpable through the generous abdominal wall, be pushed down within reach of the waiting fingers.
Slight flaring of the butt of the object allowed it to grasped by a tense claw-grip (Figure 2) of the operator’s right index and middle fingers. With firm traction estimated at about 7 kg weight over a quarter of a minute, the object came down to the anal canal and was then removed easily, followed by some blood-stained mucus. The nex day the patient, now comfortable, turned tail and hurried left the hospital.
In 1968, Orr1 of Sydney reported the case of an elderly man with an inverted glass tumbler in his rectum. Removal of the object was attempted with obstetrc forceps. The glass broke, tearing the rectum during removal, and the patient was subjected to a temperar colostomy. Others might have preferred Bacon's 2method, mentioned in the same report, in which the container was filled with plaster of Paris; possibly this method includ leaving a tail of bandage free for traction when plaster has set (orthopods should note this is still a general surgical procedure). Things previously regard as holy have been replaced by others in recent years, and other cases of this type may be expected as vibrators are sold more widely. The technique described may save laparotomy in other cases.

One concludes with a hope that this report does not end up as an amusing item in the Sunday papers, despite its comic side. The anonymity of the report does not guarantee the unfortunate subject assurance against ridicule without the use of a pseudonym.
"ERGONOME."
1 Orr, K. B., MED. J. AUST., 1968, 1: 721.
2 Bacon, H. E., Anus, Rectum, Sigmoid Colon: Diagnosis and Treatment, 3rd edition, 1949, Lippincott, Philadelphia.
-o0o-
Being a country general surgeon means you are asked to deal with a hugely wide range of surgical conditions, from a pimple or an ingrown toenail to a stab wound to the aorta and vena cava.
In between there are unusual challenges, and this description is devoted to one of them – a vibrator which was put into a young man’s rectum and then would not come out.
Faced with this problem early one Friday evening in 1974, I devised on the spot a way to remove it, which I described in a pseudonymous letter to the Medical Journal of Australia.
Basically it involved asking the anaesthetist to give the patient twice the usual dose of muscle relaxant at the start of the procedure, pressing downwards on the lower abdomen, and using a special hand-grip to retrieve the vibrator. The idea for the downward pressure with the hand was from some dimly-remembered obstetrics twenty years earlier, the so-called Crédé manouevre which is carried out to help push out the placenta if it is slow to separate and emerge.
This turned out to be only the first of several chapters that extended over several years and half-way round the world – more specifically to San Francisco, just a short hop across the Pacific River.
The first thing that happened was that the patient and his girl-friend left town earlhy the next day, doubtless from embarrassment. Early the following year another case of foreign body in the rectum, not a vibrator but an electric toothbrush which is likely to have been shorter and not as thick as a vibrator.
Med J Aust, October 19, 1974, p 615
-o0o-