Ergonomics is the scientific study of man at work. Based on knowledge of normal human capacity and structure, it is specifically concerned with the effect on human performance in work of the following factors:
(1) equipment design,
(2) workplace layout,
(3) environmental conditions such as lighting, temperature, humidity and noise, and
(4) related questions of skill acquisition, productivity, and safety.
So far, the main application of ergonomics to surgery has been to microsurgery, because of the critical nature of fine perception and movement control needed, beyond normal unaided human capacity. The range of possible applications to the mainstream of general surgery is so wide and detailed that parts of it can only be outlined briefly in the space available.
30.1 Hand grips
There are five main classes of hand grip used by surgeons:
(1) power grip, for holding large instruments with strength;
(2) external precision grip, as in writing. The instrument is at an angle
of about 45 degrees to the working surface;
(3) internal precision grip, the common scalpel grip in general surgery.
The instrument is practically parallel to the work surface. A variant
is used for scissors and ring-handled tools ;
(4) pinch grip, inappropriately termed the `precision grip' by anthropologists
and orthopaedic surgeons, for picking up small objects;
(5) ulnar storage grip, used for tucking instruments into the palm by
the ring and little fingers, while the remaining digits carry out some
other more ac-curate function. This is an element of several important
double grips of the hand useful in dissecting and suturing, which are
discussed below more fully.
Simple armchair consideration of the power grip provides about a dozen criteria for handles to fit within it. The more important are a length greater than palm width of about 12 cm, diameter of 2-3 cm to maximize skin contact area, slight flattening to control rotation without friction, flattened areas for the thumb and index for more sensitive tilt control, avoidance of sharp projections which inhibit voluntary grip strength, a small pommel and hilt to prevent slip when muscles acting on the hand relax a little, and a bend, perhaps 30 degrees, where the handle joins the shaft, to avoid ulnar deviation of the user's wrist for long periods of time.
This simple check-list helps select from alternatives available those
handle designs best suited for noo' use.
At the opposite extreme, study of the `external precision grip' of the
hand gives a basis for rational design of the microsurgical needleholder
described by Vickers. Based on the features of this hand grip. the handle
requirements are a length over 12 cm. cylindrical. shape about 1 cm in
diameter at the fingertip pulp - much thinner at the thumb cleft, and
a closing pressure fo the for the fingertips of about 50 g wt, above which
normal hand tremor becomes exaggerated.
The impact of this type of detailed analysis has been taken beyond the operator-instrument interface (the subject of ergonomics) to the instrument-tissue interface and interfaces within equipment. Vickers has elaborated further design criteria in this case, such as offset concavo-convex jaws, all based on a finely detailed consideration of surgical work.
Quite apart from handle design, hand grips and function deserve study because so much of the surgeon's work is holding tissue, peeling, and using probes, dissectors and scissors. Three examples follow.
Non-rigid tissue is best cut at right-angles to lines of tension, requiring two pulling forces, or a second re-action. A double hand grip by the operator allows him to stretch tissue in one hand while cutting it with excellent control with the other (Figure 30.1).
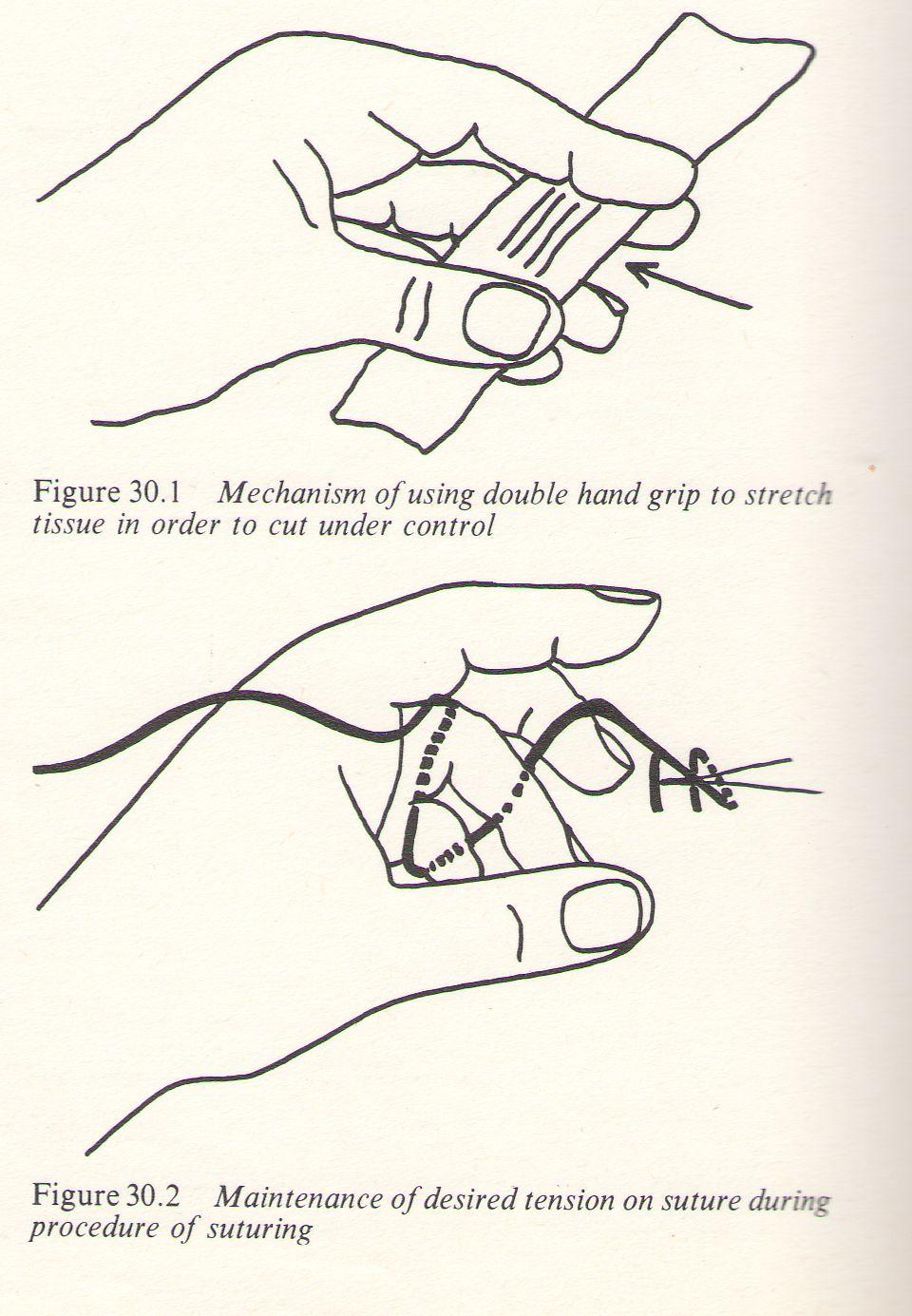
Figure 30.1 Mechanism of using double hand grip to stretch tissue in order to cut under control
Figure 30.2 Maintenance of desired tension on suture during procedure of suturing
A second example is the looping of a continuous suture from the tissue over the dorsum of the ring finger and under the palmar aspect of the flexed middle finger like a woman knitting. This lets the operator maintain the exact tension he wants on the suture while leaving the thumb and index finger free to pout open the tissue edges with-out needing an assistant, or to use dissecting forceps while holding the tissue edges apart with the bulk of his hand (Figure 30.2).
30.2 Workplace layout and organization
The best method of achieving efficient work organization is by many repetitions
of a procedure, with gradual evolution of improvements. The same operating
team carrying out many hip replacements or cleft palate repairs will achieve
a rhythm of work impossible with changing staff and infrequent procedures.
However, much can be achieved by learning, from industrial examples in
textbooks of work study, and attending to several practical factors whose
nature ranges from the very general to the detailed.
(1) Sympathetic competent leadership for example, and patience.
Repeatedly similar technique. Rehearsal of complicated new procedures.
Up-to-date cards of instruments and sutures used and special requirements
for each procedure. The minimum of gadgetry for its own sake, and simplification
of operative technique.
Attention to equipment placement and movement. based on envelopes of
reach for the arm. forceps racks designed by Sir Heneage Oglivie in 1939,
and the `drop-passage' of instruments described by H.A.F. Dudley in the
standard work Operative Surgery.
Operator seating, arm support, and operating table design remain problems
still managed by flair and in-tuition instead of scientific analysis,
despite a wealth of practical guidelines in the ergonomic literature.
With concepts already available, their application awaits only the interest
and energy of some young surgeons. It is easier for a surgeon to learn
ergonomics than for an ergonomist to learn enough surgery to bridge the
gap between the two disciplines.
30.3 Environmental conditions—lighting and vision
Studies in factories have shown the effect of environmental conditions on productivity, which is highest at a working temperature of about 18 °C, measurable humidity, and little noise. Lighting is one of the main factors which determines visual acuity and perception, and is a good example of an environmental factor to analyse for surgical work. Acuity depends on:
(1) Lighting intensity: within broad limits, visual acuity is proportional to the logarithm of the lighting intensity. Surgeons should recognize the difference between 200lx,.for desk work, and 3000 lx for an abdominal operation. Outside the operative field, the theatre sister has a problem with relatively dull lighting, especially in picking out one of several similar instruments. (There are labelling implications here.)
(2) Glare: this decreases acuity the closer is its line of incidence to the line of sight, and the brighter it is. Matt or satin finish of instruments is an advantage, though less corrosion resistant and harder to keep clean. Green drapes were introduced by Lord Moynihan early this century for such reasons, but they mask cyanosis for the anaesthetist, who now needs a white undersheet to observe the patient's colour.
(3) Colour contrast: common examples are the use of the tourniquet, methylene blue, and the attempt to use vital staining of tissues (most recently with fluorescent dyes under the operating microscope) to help discriminate structures. As in many other situations, technology is less useful than experience, but a help in its absence.
(4) Other factors important for seeing fine detail include binocularity, visual health, trained and experienced perception, magnification, the moulding effect of directional lighting, colour rendering according to the colour temperature of the light source, filters, and reflectors, flicker, and unwanted effects such as heating. Lighting levels should in-crease in proportion to magnification. A total approach would consider the ergonomics of light positioning and controls.
30.4 Skill acquisition
The manual skills of surgeons can be studied in the same way as skills in sport, industry or music. The process of skill acquisition has been divided by Glencross, at Flinders University, into three stages. Coding, the first stage, is learning to relate a particular movement to a particular end result, such as pressing middle C on the piano, or squeezing an instrument or tissue with a given amount of force. The second stage of temporal organization is the arrangement of coded movements into a sequence, such as the notes of a melody or tying a surgical knot, perhaps under the microscope. In the final stage of hierarchical organization, there is a 'pro-gramme' or `sub-routine' ready to be called on by the operator, with preliminary modifications according to other sensory input or processing, but which cannot be interrupted halfway through. It gives a smooth and rhythmic performance economical in time, if it does not have to be repeated. This is a constant feature of the skills of the best workers, artists and sportsmen.
30.5 Future developments and implications
By their temperament and training, surgeons are well equipped to make practical use of the rich existing fund of ergonomic knowledge, aided by new habits of observation concentrating on the operator and his hands and eyes, instead of on the patient, and by the use of video-tape technology now readily available. Only the stimulus for such work has been missing up till now. The application of ergonomics, in the correct context of surgical pathology, should result in better handiwork at operation, more satisfaction and less worry for the operator, and a better result for the patient.
References
Applied Ergonomics (quarterly). Guilford, Iliffe
DUDLEY, H.A.F. (1977). Operative dispositions and ergonomics. In Operative
Surgery, 3rd edn, ed. by Dudley, H.A.F., Rob, C. and Smith, R. London,
Butterworths
GLENCROSS, D.J. (1975). The control of skilled movements, Psycho/. Bull.,
84, 14-29
MURELL, K.F.H. (1965). Ergonomics: Man in His Work
ing Environment. London, Chapman & Hall PATKIN, M. (1965). The hand
has two grips: an aspect of surgical dexterity, Lancet, 1, 1384
PATKIN, M. (1967). Ergonomic aspects of surgical dexterity, Med. J. Aust.,
2, 755
PATKIN, M. (1978). Ergonomics and the operating microscope, Adv. Ophthal.,
37, 53. Basel, Karger
VICKERS, D.W. (1977). A new microsurgical needleholder, Aust. N.Z. J.
Surg., 47, (3),
-o0o-
Ergonomics and the surgeon
Clinical Science for Surgeons p578
Edited by William Burnett
MB, ChM(Aberd), FRCS, FRFPS(Glas), FRACS
Mayne Professor of Surgery, University of Queensland Member, Board of
Examiners, RACS, Chairman, Editorial Committee, Board of Examiners, RACS
Butterworths Pty. Ltd
Sydney Melbourne Brisbane Perth Adelaide
AUSTRALIA
BUTTERWORTHS PTY LTD
271-273 Lane Cove Rd, North Ryde, NSW 2113
343 Little Collins Street, Melbourne 3000
Commonwealth Bank Building, King George Square, Brisbane 4000 84 Flinders
Street, Adelaide 5000, 2nd Floor, 45 St Georges Terrace, Perth 6000
NEW ZEALAND
BUTTERWORTHS OF NEW ZEALAND LIMITED
31-35 Cumberland Place, Wellington, New Zealand ENGLAND
BUTTERWORTH & CO (PUBLISHERS) LIMITED
88 Kingsway, London WC2B 6AB SOUTH AFRICA
BUTTERWORTH & CO (SA) (PTY) LIMITED
152-154 Gale Street, Durban 4001 UNITED STATES OF AMERICA
BUTTERWORTHS (PUBLISHERS) INCORPORATED
10 Tower Office Park. Woburn. Massachusetts 01810
National Library of Australia Cataloguing-in-Publication entry
Clinical science for surgeons.
Includes index.
ISBN 0 409 49033 4.
1. Surgery. 2. Anatomy, Surgical and topographical. 3. Physiology, Pathological.
I. Burnett, William.
617
© Royal Australasian College of Surgery 1981
This book is copyright. Apart from any fair dealing for the purposes of
private study, research, criticism or review, as permitted under the Copyright
Act, no part may be reproduced by any process without written permission.
Inquiries should be addressed to the publishers.
Typeset, printed and bound in the UK
by Butler & Tanner Ltd, London and Frome.
30 Ergonomics and the surgeon Ergonomics
Michael Patkin
30.1 Hand grips 578 30.4 Skill acquisition 580
30.2 Workplace layout and organization 579 30.5 Future developments and
implications 580 30.3 Environment conditions-lighting and vision 579
-o0o-