Living things act on their environment by mechanical or chemical means. The amoeba flows to engulf a food particle and then digests It in a vacuole; birds and other larger creatures equipped with a mouth, trunk and limbs have varying abilities to push, grasp, or carry parts of their environment.
In man this manipulative function achieves its most complicated state, as Wood Jones once pointed out (1949), because of an undifferentiated hand and a highly developed part of the brain controlling It. These functions can be destroyed as completely by a stroke as by amputation.
Man, of course, goes far beyond simple manipulation to control his world. With the complexities of machines and social organization, one person can alter the state of a very large area of his environment or the conditions of millions of other people.
However, In this context I am concerned with only a single human being, his hands, and whatever simple tools he may have to perform a piece of work, particularly a surgical manoeuvre. I am concerned, too. with the wide variation in skill between one surgeon and another, and I shall use the context of ergonomics to analyse the possible basis for these differences.
Ergonomics may be defined as the study of man in relation to his working environment, and Its scope Includes such topics as the range of movement of parts of the human body and the design of instruments.top
The hand can grip things in either a powerful or a delicate way. The former is termed the power or storage grip and Is exemplified by a tennis player holding his racket. With it, mobility Is available at the wrist joint or closer to the trunk. Movement is powerful and It can be controlled to a remarkable degree as shown by the expert golfer, but It Is not suitable for small movements. It is a common static grip used, for example, In holding retractors In abdominal surgery.
The second grip of the hand, that of the fingertips, is the precision grip. It Is used typically to hold a pen or pencil. With it, movements can be controlled to the very limit of naked eye perception and beyond. Here, mobility Is at the wrist or by the coordinated movements of the thumb and fingers. It Is usual to have support for the wrist or hand because of the tremor factor, which Is analysed below.
Thus the signwriter, who has to work very deliberately, rests his working wrist on a special stick called a maulstIck, one end of which Is padded and rents on the working surface, while the other end Is held much farther away by the other hand.
Similarly, the cataract surgeon may rest three fingers on the patient's head while his thumb and index make a delicate stroke. Thus he controls his knife to a fraction of a millimetre, which would be impossible if he were to move his hand from the shoulder. In this little example lies a lesson for the general surgeon operating on smaller structures than usual.
The two grips of the hand may be used simultaneously. For ages, men have been doing more with their hands than they have appreciated. It is possible to control two separate objects In the hand at the one time, whether they are tennis balls, a whisky glass and a cigarette, or a suture and a pair of dissecting forceps.
The precision grip is not very powerful and the storage grip Is not mobile, but each has a part to play. How the surgeon can secure a suture In the storage grip by looping It behind his ring finger has already been described (Patkin, 1965)
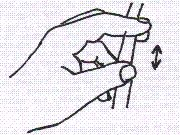
In the performance of a continuous suture this has several advantages: (i) the surgeon can use the thumb and index to expose or pout the tissue edges to receive the needle; (ii) he does not need an assistant to take up the slack; (iii) he has absolute control of the tension, which he can maintain at the desired level; (iv) he can achieve a smoother rhythm of suturing on his own; and (v) he should save time, although I cannot yet confirm this with actual records.
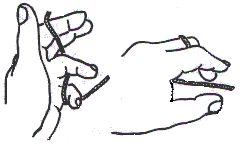
Another example Is the storage of dissecting forceps In the palm between insertions of Interrupted sutures. This saves putting the instrument down, locating it again, and picking it up. It eliminates several therbligs, or elements of motion. Yet another application of a double grip is in the cutting of tissue. Neither scissors nor knife will cut material cleanly if it Is slack and unresisting. A fundamental principle In dissection Is that the act of cutting requires lines of tension at right angles to the line of incision. It implies two secure points of attachment, one of which Is often the body. However, a ligature or mobile tissue to be cut can be secured with just one hand. One part is held between the index and middle fingers, and the other between the thumb and ring finger.top
 Figure
2.
Figure
2.
Having considered some aspects of hand function In operative surgery, I should now like to turn to the tools
wielded by the hand. Despite the many new Instrument: that are described each week In medical journals, no change of greater magnitude has occurred since the principle of the ratchet was applied to artery forceps and needleholders 90 years ago. I believe the next 10 years could see a whole new family of Instruments whose design Is based or studies in ergonomics.The Deaver retractor has been with us for many decades. Its blade provides good exposure, but it is difficult for an assistant to steady, often against heavy pressure, a handle 1 in. wide and 1/10 in. thick. In a few minutes it cuts Into the palm and makes control difficult without discomfort and strain. In approaching the ideal shape for a retractor handle there are certain principles already described which appear to be widely applicable (Patkin, 1966): (i) The handle must be sufficiently bulky to provide a good surface area of contact with the hand and fingers. (ii) It must be gently contoured to the shape of the grip with a depression for the thumb to bear down on, and a shallower groove for the opposite finger. (iii) It must be flattened from side to side to allow control of rotation. (iv) It should have a pommel at its end curving round the edge of the hand, like that on some swords and daggers. In this way the grip cannot be lost, despite momentary Insecurity. The practical test for such an instrument to that it must be comfortable and secure to hold even if wet and slippery. The milling and ridging seen on many Instruments are too fine to allow secure hold by a wet glove without undue strain. The principles of design for scissors, artery forceps and needleholders are all interesting questions for the near future.top
Needleholders versus Hand Needles
The efficiency of these two different techniques does not depend merely on the elements of motion or therbligs involved. Where tissue Is tough or thick, a hand needle Is difficult, slow, or even Impossible to use. It Is interesting to note the force with which a standard straight skin needle can be pressed against the platform of an ordinary set of bathroom scales. A hand needle can have three or tour pounds' weight exerted through It, while the use of a needleholder doubles the force that can be applied to about eight pounds' weight.
The slipperiness of gloves is a practical factor here. Mr. Norman Tanner of London (personal communication, 1965), a constant user of hand needles, has gloves with a mamillated surface. Whenever he travels abroad to demonstrate his surgical technique, he likes to take with him his own supply of "Premier" latex gloves. Strength of grip varies from one person to another and depends on practice and experience. It Is a little unfair to expect the junior or Infrequent operator to be skilful with hand needles.top
Despite the absence of published studies, manual tremor would appear to be important to surgeons, In regard to both the speed and the accuracy of their work. The basic factors establishing and varying tremor therefore deserve study.
Normal tremor of the unsupported hand has a frequency of 7 to 20 oscillations per second and an amplitude of 0.5 to 3 mm. It can be recorded In an apparatus with a light beam reflected by a hand held pointer on to a photoelectric cell which then leaves a record on a roll of sensitized paper. There are many factors which affect tremor age, sex, right and left handedness, tiredness and exhaustion or heavy muscular effort some hours before the execution of precision work, point of support of the limb, weight load on the limb. psychological factors, social poisons such as alcohol, tobacco and stimulant drugs, and such diseases an cerebral atherosclerosis, Parkinson's disease, and thyrotoxicosis.Thus the lessons of ergonomics or of common senseare that a surgeon should be physically and mentally fit, with confidence In his work, and should avoid strenuous exertion for some hours before operating. Lord Moynihan,
renowned as a smooth operator, once stated that he did not smoke cigarettes because it reduced his operating efficiency by 10%.The question of the point of limb support has already been exemplified by the signwriter using the precision grip. A further consideration is that instruments magnify tremor In proportion to their length, and for the finest vascular anastomoses a short handled Instrument Is best. It is common to see the very surface of the abdomen stitched with the use of a needle holder whose length is seven or eight Inches, though this may be merely to save adding yet another Instrument to the tray.
The Geometry of Surgical Access
Maingot's old textbook on abdominal surgery stated that in a laparotomy for intestinal obstruction the Incision must be 4.5 in. long. Simple measurement shows that the circumference of this wound, nine Inches, is also the maximum circumference of the average size 7 1/2 hand when it has been made into as small a shape as possible. Proceeding further, we find that a breast abscess usually requires exploration with the index finger, whose circumference Is two inches at its base, so therefore, the elasticity of skin being disregarded, the exploratory incision must be 1 in. long.
To generalize, the possible components of an operative space in the body comprise the following: room for the hand or fingers at rest; the volume described by movement of the hands or fingers; the volume occupied by surgical instruments at rest; the volume described by the movement of these Instruments; the conoids of binocular vision; the conoid of Illumination.
This analysis goes a step farther than describing surgical access as cramped or roomy, and may give theoretical support for the feeling that one kind of Incision Is better than another. Further, It may suggest ways of Improving access In a particular situation.
Blood Loss In Operative Surgery
This is one area where more detailed analysis along ergonomic lines must Improve operative technique. At the present time, measurements are limited to the total volume lost, although in the case of prostatectomy, further measurements have been made of the postoperative drainage.
It is important to know at what stage of an operation blood loss occurs, whether during the stage of Incision and exposure, during the early stages of dissection, during a later stage of excision, or from general oozing which has not been controlled. Further, sharper perception can indicate such obvious examples as episiotomy performed too early in the second stage of labour, or failure to clamp and ligate vascular tissue before dividing it. To paraphrase an old saying:
There's many a slip,
Betwixt cut and clip.
To decrease the glut,
Make It clip before cut.The operation of retropubic prostatectomy provides a useful example. General vascularity Is reduced a great deal by epidural anaesthesia. The skin Incision can be made bloodless by local injection with weak adrenaline solution. The capsule can be divided with very little haemorrhage by Incision a step at a time between pairs of artery forceps which are later diathermized. When most of the gland has been enucleated, it can be swung out of Its capsule postero superiorly on Its vascular pedicle derived from the inferior vesical arteries. Putting two pairs of forceps across this pedicle not only secures the main site of bleeding at this stage, but also diminishes the posterior lip of the bladder neck in the same manoeuvre. When the capsule Is finally closed, traction on the balloon catheter during the rest of the operation saves yet more bleeding. One pint of blood contains 7,500 drops, and even a Sassenach knows that "many a mickle maketh a muckle". It to with such set procedures that one of the most obvious applications of ergonomics to surgery will lie.top
The future of applying ergonomics to surgery
The advantages of quicker safe operating are numerous and obvious. Ergonomics can help especially In training our manual skill In operative surgery, not only In the early days of a surgical career, but In the retraining that goes on throughout life. An ergonomic approach will make It more obvious why one technique Is better than another, and will make It easier to learn. It Is a naked eye analysts that owes more to the tradition of Charles Darwin than to the sophisticated electronic Instruments becoming associated with surgery. Modern techniques, however, especially the videotape units now becoming generally available, will also help in the recording, analysis, and teaching of surgical skill.
It should not be long before our medical libraries stock videotapes of operative technique as a supplement to surgical textbooks. At the same time, one hopes that these libraries will have on their shelves the standard textbooks on ergonomics and time and motion study, as few doctors have ready access to such material at present. I have had to omit such standard discussion as these books contain; those who are unacquainted with flow diagrams, grasp range, therbligs, and critical mean path will find them expounded more clearly than the present opportunity allows.
There are a number of ergonomic factors of particular relevance to surgery, such as visual acuity, temperature, humidity, noise, and distractions. Published studies exist analysing these In a laboratory setting, and they must apply to operative surgery In similar ways. Surgeons have a tremendous amount to gain by Inviting experts In the field of ergonomics to visit their operating theatres, not just once or twice, but over a period of time, as they would In dealing with a factory or a business office.
The observations I have referred to do not need complicated or expensive Instruments, and they could continue for the many decades In the future In which operative surgery remains an everyday occurrence. Indeed, despite the continuing success of medicine In taking over the tasks of surgery, the horizon is constantly expanding as kidney transplants and other lengthy procedures become everyday practicalities. For such complicated reconstructions It will be even more important to achieve maximum efficiency In operating, as the incidence of many complications Is proportional to the time spent on the operating table.
Few surgeons complete a clean, safe gastrectomy In an hour as Norman Tanner does, and very few would resect an aortic aneurysm In the same time as de Bakey is reputed to. This speed is not from any great haste in individual movements, but follows efficient handicraft and simpler rather than more complicated techniques. Careful observation and thoughtfulness will allow all of us better use of that wonderful organ, the human hand. The famous French philosopher, Teilhard de Chardin, described man as a cerebro manual creature. It is the privilege of surgeons as much as any other group of people today to be able to fulfil this high and noble description. 1 must not finish without emphasizing the dominating importance In surgery of experience, good leadership, and common sense, which will achieve so much more in the future with the further exploitation of manual skill.top
I am grateful to Professor H.F.A. Dudley for the Invitation to present this paper; to Professor M. R. Ewing, for his advice about further development of these ideas; and to many surgical friends for their constructive criticism.
Referencestop
de Chardin , I. (1961), "The Phenomenon of Man", Collins, London.
Patkin M. (1965), "The Hand has Two Grips: An Aspect of Surgical Dexterity" Lancet, 1 : 1384.
Patkin M. (1966), "The Shape of Retractor Handles", MED. J. AUST., 1 : 599.
Maingot R. (1936), "Modern Operative Surgery", Butterworth, London, Vol. 1.
Wood Jones F. (1949), "Principles of Anatomy as Seen In the Hand", 2nd Edition, Bailliere, Tindall & Cox, London.
-o0o-
Contents
The hand has two grips
Instruments
Handle design
Needleholders versus hand needles
Problems of surgery
Tremor and operative surgery
The geometry of surgical access
Blood loss in operative surgery
The future of applying ergonomics to surgery
Acknowledgements
References
Ergonomic Aspects of Surgical Dexterity
MICHAEL PATKIN, F.R.C.S., F.R.C.S. (Edin.), F.R.A.C.S.2
Dungog, N.S.W.
Reprinted from The Medical Journal of Australia, 1967, 2: 775 (October 21)
[1] Part of a symposium on Biological Engineering and
Surgery hold at the Department of Surgery, Monash University, May 26,
1967.
[2] Honorary Medical Officer, Dungog and District Hospital, N.S.W. 2420.
_______________________________
Being in a small country town at the time it may seem surprising I was asked to speak at this high-level gathering.
However I had written to Professor HAF (Hugh) Dudley, foundation professor of surgery at Monash University, with admiration for and interest in his recent book on Access and Exposure in Abdominal Surgery.
I included references to my 1995 paper on hand grips in the Lancet and recent thoughts and explorations of mine on ergonomics. As a result there followed the invitation to speak and the opportunity to meet top-level stars in surgery and bioengineering, such as Gibson, the plastic surgeon from Strathclyde, a current major centre in bio-engineering. An example of this was research on modelling of skin deformation using classical work on elasticity and its equations.
-o0o-